Moving a patient from bed to wheelchair is a routine but high-risk caregiving task that demands precision, proper technique, and the right tools. Done incorrectly, it can lead to serious injuries—over 50% of nursing staff report back pain from unsafe patient handling, and falls during transfers are a leading cause of hospital-acquired harm. Whether you’re a professional caregiver in a clinical setting or a family member providing home care, knowing how to move a patient from bed to wheelchair using safe, evidence-based methods is essential for protecting both the patient and yourself.
This guide breaks down the entire transfer process into clear, actionable steps using three primary techniques: gait belt-assisted pivot transfer, transfer board slide, and mechanical lift use. You’ll learn how to assess the patient’s ability, prepare the environment, choose the correct equipment, and execute each transfer with confidence. By following these best practices, you ensure dignity, reduce injury risks, and support patient independence.
Assess Patient Mobility Before Any Transfer
Never assume a patient can stand or pivot—always evaluate first. The wrong method can result in falls, joint strain, or caregiver injury.
Can the Patient Bear Weight on Their Legs?
Ask the patient to:
– Sit up without help.
– Scoot to the edge of the bed.
– Push up with their arms or stand briefly.
If they struggle or cannot do this, they are non-weight-bearing and require a mechanical lift.
Test Upper Body Strength and Balance
Have the patient push down on the bed with both hands. Weak arm strength means they can’t assist in a pivot or slide transfer.
Check sitting balance: Does the patient wobble or lean when upright? Poor trunk control increases fall risk and requires full mechanical support.
Review Medical Restrictions
Certain conditions dictate transfer limitations:
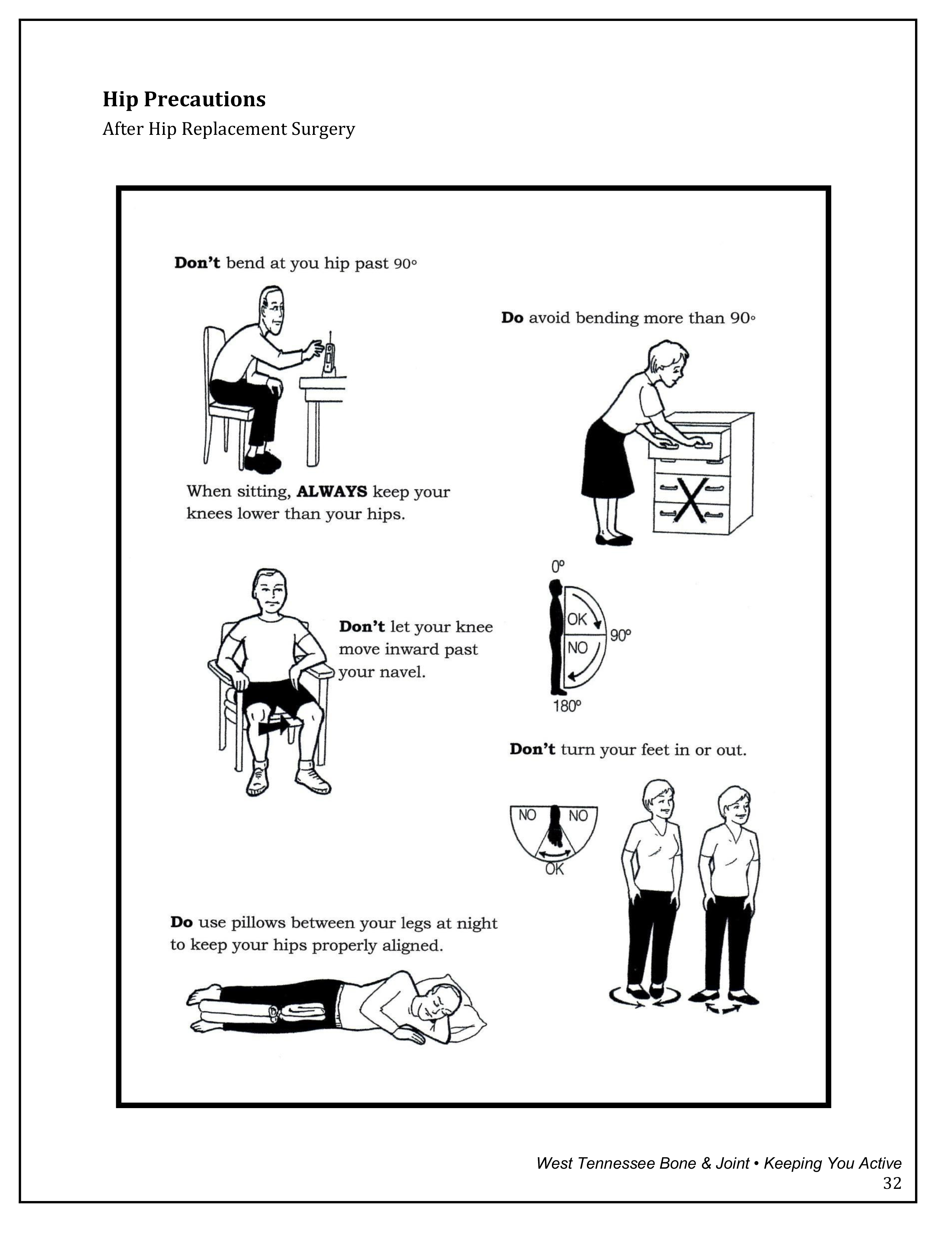
– After hip replacement, avoid bending the hip past 90° or twisting inward.
– With spinal injuries, use log-rolling and no torso rotation.
– Orthostatic hypotension causes dizziness when sitting up—allow 1–2 minutes at the edge of the bed before proceeding.
Patients who are confused, uncooperative, or unconscious should never be manually transferred. Use a mechanical lift instead.
Prepare the Room and Equipment Properly
A rushed setup leads to avoidable accidents. Take time to create a safe, obstacle-free environment.
Clear the Path Between Bed and Wheelchair
Remove IV poles, loose rugs, or clutter. Ensure at least 30–36 inches of clearance for maneuvering. Check that the floor is dry and non-slip—wet or waxed surfaces increase fall risk significantly.
Position the Wheelchair Correctly
- Lock the brakes immediately.
- Swing away or remove armrests to allow easy seating.
- Elevate or detach footrests before the transfer.
- Adjust seat height to be level with or slightly lower than the bed.
- For pivot transfers, place the wheelchair at a 45-degree angle to the bed. For board or lift transfers, position it directly beside the bed.
Choose and Use the Right Transfer Device

The device you use must match the patient’s mobility level and physical condition.
Apply a Gait Belt the Right Way
A gait belt gives you control without grabbing clothing or limbs.
- Place it around the waist, just above the hip bones (iliac crests), with the buckle in front.
- Tighten so two fingers fit underneath—snug but not constricting.
- Avoid placing over wounds, surgical sites, or feeding tubes.
- Only use with patients who can bear weight and assist in standing.
Set Up a Transfer Board for Sliding
Ideal for patients with leg weakness but good upper body strength.
- Use a smooth, non-slip board long enough to bridge bed and wheelchair.
- Slide one end under the patient’s buttocks while seated.
- Rest the other end securely on the wheelchair seat.
- Hold the board steady during the transfer to prevent slipping.
Prepare a Mechanical Lift and Sling
For fully dependent or non-weight-bearing patients.
- Choose the correct sling:
- Full-body for general use.
- Hemi-sling for stroke patients with one-sided weakness.
- Bariatric sling for higher weight capacity.
- Gently roll the patient to one side and slide the sling under, ensuring:
- Head end supports the upper back.
- Tail extends beyond the buttocks.
- Re-center the patient once the sling is in place.
- Position the lift under the bed, lock wheels, and attach sling loops to the spreader bar—double-check all connections.
Perform a Gait Belt-Assisted Pivot Transfer
Use this method when the patient can stand and pivot with help.
Seat the Patient at the Edge of the Bed
Help them scoot forward until feet are flat on the floor, knees bent slightly below 90 degrees.
Allow them to sit for 1–2 minutes to prevent dizziness from orthostatic hypotension. Ask: “Do you feel dizzy or lightheaded?”
Stand in a Stable Position
Face the patient, feet shoulder-width apart, one foot slightly behind their leg for balance.
Maintain hip-to-hip contact—never stand directly in front where you could be pulled off balance.
Guide the Patient to Stand
Instruct: “Lean forward, head up, back straight.”
On a count of three, say: “Stand up now.”
Grasp the gait belt firmly at the sides, keep your back straight, and use your legs to help lift.
Do not pull with your arms or twist your spine.
Pivot Toward the Wheelchair
If one side is weaker, have the patient pivot on their stronger foot.
You pivot with them, staying close and guiding with the belt.
Use clear cues: “Step with your right foot,” “Turn now.”
Lower Into the Wheelchair
Back the patient up until their legs touch the wheelchair.
Say: “Reach for the armrests.”
Grasp the belt at the center of the back and guide a slow, controlled sit-down.
Ensure hips are fully back in the seat before releasing the belt.
Execute a Transfer Board Slide
Use when the patient can’t stand but has upper body strength.
Position the Board Correctly
With the patient seated at the edge, slide the board under their thighs and buttocks.
The other end rests firmly on the wheelchair seat.
Stabilize the board with one hand to prevent shifting.
Instruct the Patient to Slide Across
Say: “Lean forward and push with your hands on the bed.”
Support with the gait belt or shoulders—do not pull.
Let the patient control the pace.
Remove the Board and Adjust Positioning
Once fully seated, carefully slide the board out.
Reposition legs on footrests and ensure proper posture.
Operate a Mechanical Lift Without Risk
This is the safest option for dependent or high-risk patients.
Lift the Patient Slowly Off the Bed
Engage the lift control to raise the patient a few inches.
Pause to check:
– Sling is secure and not twisted.
– Patient is comfortable.
– No clothing or tubing is caught.
Move the Patient Over to the Wheelchair
Steer the lift carefully toward the wheelchair.
A second caregiver should guide the patient and stabilize the base.
Align the patient’s hips with the center of the wheelchair seat.
Lower Gently Into the Seat
Gradually lower until the patient is fully seated.
Ensure feet clear the footrests, which should be ready for placement.
Once down, detach the sling from the spreader bar.
Remove the Sling Safely
Roll the patient gently to one side and slide the sling out.
Repeat on the other side if needed.
Never drag the sling—this can cause skin shearing or pressure injuries.
Prevent Falls and Protect Yourself
Safety starts before the transfer begins and continues until the patient is secure.
Lock All Brakes—Every Time
Confirm:
– Bed brakes are locked.
– Wheelchair brakes are engaged.
– Lift casters are secured.
One unlocked wheel can lead to a serious fall.
Use Proper Body Mechanics
Protect your back by:
– Keeping your spine straight.
– Bending your knees, not your waist.
– Avoiding twisting motions.
– Using leg strength, not arm pull.
If you feel strain, stop and use a lift or call for help.
Never Attempt Unsafe Manual Transfers
Avoid manual lifting if the patient:
– Cannot bear weight.
– Weighs more than you can safely support (typically >35 lbs of unsupported weight).
– Has unstable medical conditions.
The risk of injury is too high.
Finalize Positioning and Document the Transfer
After the transfer, ensure comfort, safety, and proper alignment.
Adjust Posture in the Wheelchair
- Scoot hips fully back into the seat.
- Position knees at 90 degrees.
- Place feet flat on footrests—never let them dangle.
- Fasten any seatbelt or positioning strap if needed.
- Add a gel or foam cushion for pressure relief, especially for patients at risk of pressure ulcers.
Reset Equipment and Inspect for Damage
- Return the bed to its lowest safe position.
- Store the gait belt, board, or lift per facility guidelines.
- Check all equipment for fraying, cracks, or contamination.
Monitor the Patient and Document Key Details
Accurate documentation supports care continuity and identifies risks.
Record in Patient Notes:
- Type of transfer used.
- Level of assistance (independent, minimal, moderate, maximal, total).
- Patient tolerance (e.g., “tolerated well,” “complained of dizziness”).
- Any difficulties or safety concerns.
Watch for Warning Signs
After transfer, monitor for:
– Dizziness or lightheadedness.
– Pain in hips, back, or surgical sites.
– Skin redness over bony areas.
Report changes immediately.
Adapt for Special Patient Conditions
Tailor your approach based on diagnosis and limitations.
Hip Replacement Patients
Follow surgeon orders:
– No hip flexion beyond 90 degrees.
– No crossing legs.
– Use abduction pillow or hemi-lift sling.
– Prefer mechanical lifts early in recovery.
Stroke or Hemiparesis
- Support the weaker side with your hand on the gait belt.
- Encourage use of the strong leg to pivot.
- Use a transfer board for added stability.
- Provide clear, simple verbal cues.
Bariatric Patients
- Use bariatric-rated lifts and slings.
- Ensure wheelchair supports the patient’s weight.
- Require two trained caregivers.
- Check floor load capacity in home settings.
Train, Follow Protocols, and Avoid Common Mistakes
Safe transfers require knowledge, practice, and teamwork.
Get Proper Training
All caregivers should complete Safe Patient Handling (SPH) training and annual competency checks.
Avoid These Common Errors
- Rushing the process—allow time for dizziness to resolve.
- Letting the patient grab your neck—instruct them to hold armrests or your shoulders without pulling.
- Skipping the dizziness check—always pause after sitting up.
Summary: Key Takeaways
- Assess first: Mobility, strength, and medical status determine the method.
- Prepare thoroughly: Clear space, lock brakes, position equipment.
- Use the right device: Gait belt for assisted pivots, board for sliding, lift for dependent patients.
- Protect yourself: Bend knees, keep back straight, avoid twisting.
- Prioritize safety: Never manually lift non-weight-bearing patients.
- Position correctly: Hips back, feet supported, posture aligned.
- Document everything: Transfer type, assistance level, patient response.
Mastering how to move a patient from bed to wheelchair safely ensures dignity, prevents injury, and supports independence. Whether in a hospital, nursing home, or home care, following these best practices leads to better outcomes for everyone involved.